
იმუნოჰისტოქიმიური მარკერების SOX2-ის, Ki67-ისა და p53-ის ექსპრესიის თავისებურებები ბარეტის საყლაპავის, დისპლაზიასა და ადენოკარცინომამდე პროგრესირებაში

ჩამოტვირთვები




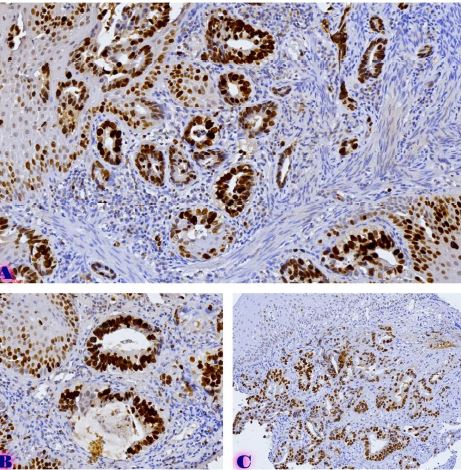
ბარეტის საყლაპავი (BE) არის სიმსივნისწინარე მდგომარეობა, რომელიც საყლაპავის ადენოკარცინომამდე (EAC) პროგრესირებს სხვადასხვა ხარისხის დისპლაზიური ცვლილებების თანმიმდევრობით. მოლეკულური ცვლილებები, რომლებიც მონაწილეობს ამ ტრანსფორმაციაში, ბოლომდე არ არის კარგად შესწავლილი. ჩვენი კვლევა ავლენს SOX2, Ki67 და p53-ის ექსპრესიის თავისებურებებს ბარეტის საყლაპავის პროგრესირების სხვადასხვა ეტაპებზე იმუნოჰისტოქიმიური კვლევის ტექნოლოგიის გამოყენებით. კვლევის ფარგლებში ჩატარებულია რეტროსპექტული კოჰორტული ანალიზი 90 ფორმალინში ფიქსირებულ და პარაფინით ჩაყალიბებულ (FFPE) ქსოვილის ნიმუშზე პაციენტებიდან, რომლებიც დიაგნოსტირებული იყვნენ ექვს საკვლევ ჯგუფად: ნორმალური საყლაპავის ბრტყელი ეპითელიუმი (n=15), რეფლუქსური დაავადება (n=15), არადისპლასზიური BE (n=15, მაღალი ხარისხის (n=15), დაბალი ხარისხის (n=15) დისპლაზია და საყლაპავის ადენოკარცინომა (EAC, n=15). კვლევის შედეგებმა აჩვენა, რომ SOX2-ის ექსპრესია მნიშვნელოვნად შემცირდა დაავადების პროგრესირებასთან ერთად (p <0.001), ძლიერი ექსპრესიით საყლაპავის ნორმალურ ეპითელიუმში (58.3 ± 4.8%) და თითქმის მთლიანი დაკარგვით EAC-ში. Ki67-ის ექსპრესია მნიშვნელოვნად გაიზარდა დისპლაზიურ და სიმსივნურ ქსოვილებში (p <0.001), ყველაზე მაღალი დონე დაფიქსირდა HGD-ში (38.3 ± 4.8%). p53 ბირთვული ექსპრესია მინიმალური იყო ნორმალურ და არადისპლაზიურ BE-ში, მაგრამ მნიშვნელოვნად გაიზარდა HGD-ში (35.0 ± 11.2%) და პიკს მიაღწია EAC-ში (53.3 ± 9.7%) (p <0.001), რაც მიუთითებს TP53 მუტაციის ჩართვაზე ავთვისებიან ტრანსფორმაციაში. კვლევის შედეგად არსებული მონაცემების საფუძველზე შეგვიძლია ვივარაუდოთ, რომ SOX2-ის დაქვეითება ადრეული მოვლენაა BE-ში, რაც ხელს უწყობს ნაწლავის მეტაპლაზიას, ხოლო Ki67 და p53-ის ჭარბი ექსპრესია დაკავშირებულია დისპლაზიის პროგრესირებასთან. ეს ბიომარკერები შეიძლება იყოს სასარგებლო ინდიკატორები მაღალი რისკის მქონე პაციენტების იდენტიფიცირებისთვის, რომლებიც საჭიროებენ უფრო აქტიურ მეთვალყურეობას და მკურნალობის ადრეულ სტრატეგიებს.
Downloads
P. Meshveliani, G. Didava, G. Tomadze, S. Kepuladze, and G. Burkadze, “Evaluation of proliferative activity of pre-tumor and tumor processes of Barrett’s esophagus using AgNor technology,” ქართველი მეცნიერები, vol. 5, no. 2, pp. 49–62, Apr. 2023, doi: 10.52340/gs.2023.05.02.07.
G. A. Prasad, A. Bansal, P. Sharma, and K. K. Wang, “Predictors of Progression in Barrett’s Esophagus: Current Knowledge and Future Directions,” Am J Gastroenterol, vol. 105, no. 7, p. 1490, Jul. 2010, doi: 10.1038/AJG.2010.2.
N. Vakil et al., “The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus,” American Journal of Gastroenterology, vol. 101, no. 8, Aug. 2006, doi: 10.1111/J.1572-0241.2006.00630.X.
B. F. Overholt et al., “Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett’s esophagus: International, partially blinded, randomized phase III trial,” Gastrointest Endosc, vol. 62, no. 4, pp. 488–498, Oct. 2005, doi: 10.1016/J.GIE.2005.06.047.
L. M. Dong et al., “Dietary supplement use and risk of neoplastic progression in esophageal adenocarcinoma: A prospective study,” Nutr Cancer, vol. 60, no. 1, pp. 39–48, Jan. 2008, doi: 10.1080/01635580701586762.
C. L. Ogden, S. Z. Yanovski, M. D. Carroll, and K. M. Flegal, “The Epidemiology of Obesity,” Gastroenterology, vol. 132, no. 6, pp. 2087–2102, 2007, doi: 10.1053/J.GASTRO.2007.03.052.
Z. R. Edelstein, D. C. Farrow, M. P. Bronner, S. N. Rosen, and T. L. Vaughan, “Central Adiposity and Risk of Barrett’s Esophagus,” Gastroenterology, vol. 133, no. 2, pp. 403–411, 2007, doi: 10.1053/J.GASTRO.2007.05.026.
L. C. Hillman, L. Chiragakis, B. Shadbolt, G. L. Kaye, and A. C. Clarke, “Proton-pump inhibitor therapy and the development of dysplasia in patients with Barrett’s oesophagus,” Medical Journal of Australia, vol. 180, no. 8, pp. 387–391, Apr. 2004, doi: 10.5694/J.1326-5377.2004.TB05991.X.
J. Jankowski and H. Barr, “Improving surveillance for Barrett’s oesophagus: AspECT and BOSS trials provide an evidence base [11],” Br Med J, vol. 332, no. 7556, p. 1512, Jun. 2006, doi: 10.1136/BMJ.332.7556.1512.
T. Kveliashvili, G. Didava, S. Kepuladze, and G. Burkadze, “Problematic issues of the mucous membrane inflammatory changes of the gallbladder and the features of hormonal expression in the development of dysplasia-carcinoma consequence,” ქართველი მეცნიერები, vol. 4, no. 5, pp. 108–119, Oct. 2022, doi: 10.52340/gs.2022.04.05.13.
T. Kveliashvili, დიდავაგიორგი, თევზაძენინო, კეპულაძეშოთა, and ბურკაძეგიორგი, “Peculiarities of the proliferative activity of the gallbladder mucosa in precancerous and cancerous pathologies detected by AgNOR technology,” ქართველი მეცნიერები, vol. 5, no. 4, pp. 342–352, Dec. 2023, doi: 10.52340/gs.2023.05.04.31.
E. Y. Chang et al., “The effect of antireflux surgery on esophageal carcinogenesis in patients with barrett esophagus: A systematic review,” Ann Surg, vol. 246, no. 1, pp. 11–21, Jul. 2007, doi: 10.1097/01.SLA.0000261459.10565.E9.
K. E. Corey, S. M. Schmitz, and N. J. Shaheen, “Does a Surgical Antireflux Procedure Decrease the Incidence of Esophageal Adenocarcinoma in Barrett’s Esophagus? A Meta-Analysis,” American Journal of Gastroenterology, vol. 98, no. 11, pp. 2390–2394, 2003, doi: 10.1111/J.1572-0241.2003.08702.X.
L. Lundell et al., “Comparing laparoscopic antireflux surgery with esomeprazole in the management of patients with chronic gastro-oesophageal reflux disease: A 3-year interim analysis of the LOTUS trial,” Gut, vol. 57, no. 9, pp. 1207–1213, Sep. 2008, doi: 10.1136/GUT.2008.148833.
P. Parrilla et al., “Long-Term Results of a Randomized Prospective Study Comparing Medical and Surgical Treatment of Barrett’s Esophagus,” Ann Surg, vol. 237, no. 3, pp. 291–298, 2003, doi: 10.1097/01.SLA.0000055269.77838.8E.
A. P. Weston et al., “Risk stratification of Barrett’s esophagus: Updated prospective multivariate analysis,” American Journal of Gastroenterology, vol. 99, no. 9, pp. 1657–1666, Sep. 2004, doi: 10.1111/J.1572-0241.2004.30426.X.
P. C. Galipeau et al., “NSAIDs modulate CDKN2A, TP53, and DNA content risk for progression to esophageal adenocarcinoma,” PLoS Med, vol. 4, no. 2, pp. 0342–0353, Feb. 2007, doi: 10.1371/JOURNAL.PMED.0040067.
R. Kariv et al., “The Seattle Protocol Does Not More Reliably Predict the Detection of Cancer at the Time of Esophagectomy Than a Less Intensive Surveillance Protocol,” Clinical Gastroenterology and Hepatology, vol. 7, no. 6, pp. 653–658, Jun. 2009, doi: 10.1016/J.CGH.2008.11.024.
S. Wani, S. Mathur, and P. Sharma, “How to Manage a Barrett’s Esophagus Patient With Low-Grade Dysplasia,” Clinical Gastroenterology and Hepatology, vol. 7, no. 1, pp. 27–32, 2009, doi: 10.1016/J.CGH.2008.08.014.
A. Rastogi, S. Puli, H. B. El-Serag, A. Bansal, S. Wani, and P. Sharma, “Incidence of esophageal adenocarcinoma in patients with Barrett’s esophagus and high-grade dysplasia: a meta-analysis,” Gastrointest Endosc, vol. 67, no. 3, pp. 394–398, Mar. 2008, doi: 10.1016/J.GIE.2007.07.019.
M. Skacel, R. E. Petras, T. L. Gramlich, J. E. Sigel, J. E. Richter, and J. R. Goldblum, “The Diagnosis of Low-Grade Dysplasia in Barrett’s Esophagus and Its Implications for Disease Progression,” American Journal of Gastroenterology, vol. 95, no. 12, pp. 3383–3387, Dec. 2000, doi: 10.1111/J.1572-0241.2000.03348.X.
საავტორო უფლებები (c) 2025 ქართველი მეცნიერები

ეს ნამუშევარი ლიცენზირებულია Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 საერთაშორისო ლიცენზიით .
