
Immunohistochemical Analysis of SOX2, Ki67, and p53 Expression in the Progression of Barrett’s Esophagus to Esophageal Adenocarcinoma

Downloads




Background: Barrett’s esophagus (BE) is a premalignant condition that progresses to esophageal adenocarcinoma (EAC) through a sequence of dysplastic changes. The molecular alterations involved in this transition remain incompletely understood. This study evaluates the expression of SOX2, Ki67, and p53 across different stages of BE progression using immunohistochemistry.
Methods: A retrospective analysis was performed on 90 formalin-fixed paraffin-embedded (FFPE) tissue samples from patients categorized into six groups: normal esophageal squamous epithelium (n=15), reflux disease (n=15), non-dysplastic BE (n=15), low-grade dysplasia (LGD, n=15), high-grade dysplasia (HGD, n=15), and esophageal adenocarcinoma (EAC, n=15). Immunohistochemical staining for SOX2, Ki67, and p53 was conducted. Staining intensity and percentage of positive cells were assessed semi-quantitatively. Statistical analysis was performed using ANOVA and Spearman’s correlation tests.
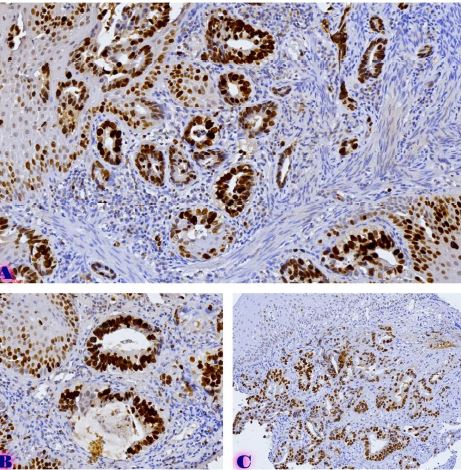
Results: SOX2 expression was significantly reduced with disease progression (p < 0.001), with strong expression in normal esophageal epithelium (58.3 ± 4.8%) and near-total loss in EAC. Ki67 expression increased significantly in dysplastic and neoplastic tissues (p < 0.001), with the highest levels observed in HGD (38.3 ± 4.8%). p53 nuclear accumulation was minimal in normal and non-dysplastic BE, but increased significantly in HGD (35.0 ± 11.2%) and peaked in EAC (53.3 ± 9.7%) (p < 0.001), suggesting TP53 mutation involvement in malignant transformation.
Conclusion: The findings suggest that SOX2 downregulation is an early event in BE, facilitating intestinal metaplasia, while Ki67 and p53 overexpression are associated with dysplasia progression. These biomarkers may serve as useful indicators for identifying high-risk BE patients requiring closer surveillance and early intervention strategies.
Downloads
P. Meshveliani, G. Didava, G. Tomadze, S. Kepuladze, and G. Burkadze, “Evaluation of proliferative activity of pre-tumor and tumor processes of Barrett’s esophagus using AgNor technology,” ქართველი მეცნიერები, vol. 5, no. 2, pp. 49–62, Apr. 2023, doi: 10.52340/gs.2023.05.02.07.
G. A. Prasad, A. Bansal, P. Sharma, and K. K. Wang, “Predictors of Progression in Barrett’s Esophagus: Current Knowledge and Future Directions,” Am J Gastroenterol, vol. 105, no. 7, p. 1490, Jul. 2010, doi: 10.1038/AJG.2010.2.
N. Vakil et al., “The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus,” American Journal of Gastroenterology, vol. 101, no. 8, Aug. 2006, doi: 10.1111/J.1572-0241.2006.00630.X.
B. F. Overholt et al., “Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett’s esophagus: International, partially blinded, randomized phase III trial,” Gastrointest Endosc, vol. 62, no. 4, pp. 488–498, Oct. 2005, doi: 10.1016/J.GIE.2005.06.047.
L. M. Dong et al., “Dietary supplement use and risk of neoplastic progression in esophageal adenocarcinoma: A prospective study,” Nutr Cancer, vol. 60, no. 1, pp. 39–48, Jan. 2008, doi: 10.1080/01635580701586762.
C. L. Ogden, S. Z. Yanovski, M. D. Carroll, and K. M. Flegal, “The Epidemiology of Obesity,” Gastroenterology, vol. 132, no. 6, pp. 2087–2102, 2007, doi: 10.1053/J.GASTRO.2007.03.052.
Z. R. Edelstein, D. C. Farrow, M. P. Bronner, S. N. Rosen, and T. L. Vaughan, “Central Adiposity and Risk of Barrett’s Esophagus,” Gastroenterology, vol. 133, no. 2, pp. 403–411, 2007, doi: 10.1053/J.GASTRO.2007.05.026.
L. C. Hillman, L. Chiragakis, B. Shadbolt, G. L. Kaye, and A. C. Clarke, “Proton-pump inhibitor therapy and the development of dysplasia in patients with Barrett’s oesophagus,” Medical Journal of Australia, vol. 180, no. 8, pp. 387–391, Apr. 2004, doi: 10.5694/J.1326-5377.2004.TB05991.X.
J. Jankowski and H. Barr, “Improving surveillance for Barrett’s oesophagus: AspECT and BOSS trials provide an evidence base [11],” Br Med J, vol. 332, no. 7556, p. 1512, Jun. 2006, doi: 10.1136/BMJ.332.7556.1512.
T. Kveliashvili, G. Didava, S. Kepuladze, and G. Burkadze, “Problematic issues of the mucous membrane inflammatory changes of the gallbladder and the features of hormonal expression in the development of dysplasia-carcinoma consequence,” ქართველი მეცნიერები, vol. 4, no. 5, pp. 108–119, Oct. 2022, doi: 10.52340/gs.2022.04.05.13.
T. Kveliashvili, დიდავაგიორგი, თევზაძენინო, კეპულაძეშოთა, and ბურკაძეგიორგი, “Peculiarities of the proliferative activity of the gallbladder mucosa in precancerous and cancerous pathologies detected by AgNOR technology,” ქართველი მეცნიერები, vol. 5, no. 4, pp. 342–352, Dec. 2023, doi: 10.52340/gs.2023.05.04.31.
E. Y. Chang et al., “The effect of antireflux surgery on esophageal carcinogenesis in patients with barrett esophagus: A systematic review,” Ann Surg, vol. 246, no. 1, pp. 11–21, Jul. 2007, doi: 10.1097/01.SLA.0000261459.10565.E9.
K. E. Corey, S. M. Schmitz, and N. J. Shaheen, “Does a Surgical Antireflux Procedure Decrease the Incidence of Esophageal Adenocarcinoma in Barrett’s Esophagus? A Meta-Analysis,” American Journal of Gastroenterology, vol. 98, no. 11, pp. 2390–2394, 2003, doi: 10.1111/J.1572-0241.2003.08702.X.
L. Lundell et al., “Comparing laparoscopic antireflux surgery with esomeprazole in the management of patients with chronic gastro-oesophageal reflux disease: A 3-year interim analysis of the LOTUS trial,” Gut, vol. 57, no. 9, pp. 1207–1213, Sep. 2008, doi: 10.1136/GUT.2008.148833.
P. Parrilla et al., “Long-Term Results of a Randomized Prospective Study Comparing Medical and Surgical Treatment of Barrett’s Esophagus,” Ann Surg, vol. 237, no. 3, pp. 291–298, 2003, doi: 10.1097/01.SLA.0000055269.77838.8E.
A. P. Weston et al., “Risk stratification of Barrett’s esophagus: Updated prospective multivariate analysis,” American Journal of Gastroenterology, vol. 99, no. 9, pp. 1657–1666, Sep. 2004, doi: 10.1111/J.1572-0241.2004.30426.X.
P. C. Galipeau et al., “NSAIDs modulate CDKN2A, TP53, and DNA content risk for progression to esophageal adenocarcinoma,” PLoS Med, vol. 4, no. 2, pp. 0342–0353, Feb. 2007, doi: 10.1371/JOURNAL.PMED.0040067.
R. Kariv et al., “The Seattle Protocol Does Not More Reliably Predict the Detection of Cancer at the Time of Esophagectomy Than a Less Intensive Surveillance Protocol,” Clinical Gastroenterology and Hepatology, vol. 7, no. 6, pp. 653–658, Jun. 2009, doi: 10.1016/J.CGH.2008.11.024.
S. Wani, S. Mathur, and P. Sharma, “How to Manage a Barrett’s Esophagus Patient With Low-Grade Dysplasia,” Clinical Gastroenterology and Hepatology, vol. 7, no. 1, pp. 27–32, 2009, doi: 10.1016/J.CGH.2008.08.014.
A. Rastogi, S. Puli, H. B. El-Serag, A. Bansal, S. Wani, and P. Sharma, “Incidence of esophageal adenocarcinoma in patients with Barrett’s esophagus and high-grade dysplasia: a meta-analysis,” Gastrointest Endosc, vol. 67, no. 3, pp. 394–398, Mar. 2008, doi: 10.1016/J.GIE.2007.07.019.
M. Skacel, R. E. Petras, T. L. Gramlich, J. E. Sigel, J. E. Richter, and J. R. Goldblum, “The Diagnosis of Low-Grade Dysplasia in Barrett’s Esophagus and Its Implications for Disease Progression,” American Journal of Gastroenterology, vol. 95, no. 12, pp. 3383–3387, Dec. 2000, doi: 10.1111/J.1572-0241.2000.03348.X.
Copyright (c) 2025 Georgian Scientists

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
