HYPOVOLEMIC SHOCK – DIAGNOSTIC CHALLENGES AND EFFECTIVE MANAGEMENT STRATEGIES (CASE DISCUSSION)

Downloads




Pediatric shock is a leading contributor to global mortality and morbidity in children. Because children maintain compensated physiology until late stages, the presence of hypotension signals immediate decompensation, necessitating rapid and decisive management. The principal obstacle is the broad variation in age-dependent hemodynamic parameters and pharmaceutical dosing, often leading to errors and non-standardized care, particularly in general hospital settings. A consolidated, practical methodology for clinicians is essential. This investigation sought to construct an innovative, synthesized educational and procedural framework for pediatric hypotensive shock, integrating fundamental global protocols (PALS, SSC) into a unified algorithm to optimize clinical response time.
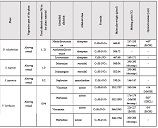
Methods: We performed a focused narrative synthesis of established international clinical guidelines, notably the 2020 AHA PALS and the 2020 Surviving Sepsis Campaign Pediatric Guidelines. The resulting framework organizes treatment around three specific physiological groups: infants (0–12 months), young children (1–5 years), and school-age children (6–12 years). The derived protocol details sequential management, from early detection and initial volume expansion (20 mL/kg fluid boluses) to the critical juncture of initiating pharmacologic support. A dual-citation method is utilized to robustly link clinical steps to their evidence base.
The framework precisely defined minimal intervention thresholds for systolic blood pressure based on age, such as < 70 mmHg for infants and < 70 + (2 x Age in Years) mmHg for older pediatric patients. Crucially, the selection of the initial vasoactive agent was tailored to the presumed shock profile: Epinephrine or Dopamine was prioritized for infants (0–12 months) due to prevalence of "cold shock," while Norepinephrine was favored for school-age children (6–12 years), aligning with protocols emphasizing direct vasopressor action for generalized vasodilation ("warm shock"). This clear differentiation significantly diminishes clinical ambiguity and error potential.
Conclusion: This newly developed age-adjusted training framework delivers an efficient, evidence-supported strategy for prompt pediatric shock stabilization. This unified approach effectively minimizes the occurrence of dosing and protocol deviations, proving highly beneficial for both critical care education and adherence to guidelines in diverse clinical environments.
Downloads
Copyright (c) 2025 Georgian Scientists

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.