SARCOPENIC CONDITION INDUCED BY SEPSIS IN ACUTE RESPIRATORY DISTRESS SYNDROME

Downloads




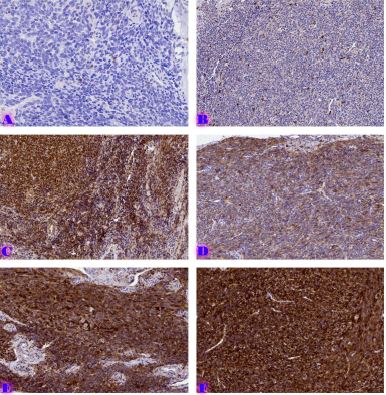
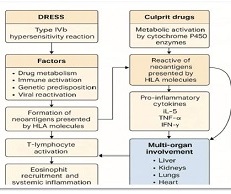
Sepsis remains a major cause of morbidity and mortality among critically ill patients and is frequently complicated by multiple organ dysfunction, including acute respiratory distress syndrome (ARDS) and severe skeletal muscle wasting, known as sepsis-associated sarcopenia. ARDS is a form of non-cardiogenic respiratory failure characterized by diffuse alveolar damage, increased capillary permeability, and refractory hypoxemia requiring advanced ventilatory support. Its pathogenesis in sepsis involves a dysregulated immune response in which pathogen- and damage-associated molecular patterns trigger toll-like receptor signaling and nuclear factor-κB–mediated transcription of pro-inflammatory cytokines. This cascade disrupts endothelial and epithelial barriers, promotes neutrophil infiltration, and leads to oxidative tissue injury and surfactant dysfunction, resulting in impaired gas exchange and decreased lung compliance.
Simultaneously, sepsis induces profound metabolic and hormonal disturbances that accelerate skeletal muscle catabolism. Elevated cytokines such as tumor necrosis factor-α, interleukin-1β, and interleukin-6 inhibit anabolic signaling and suppress the mechanistic target of rapamycin (mTOR) pathway, thereby reducing protein synthesis. Activation of forkhead box O (FOXO) transcription factors enhances the expression of muscle-specific E3 ubiquitin ligases, MuRF1 and Atrogin-1, which drive proteasome-mediated degradation of contractile proteins. Mitochondrial dysfunction and impaired oxidative phosphorylation further contribute to muscle fatigue and atrophy, while autophagy–lysosome activity exacerbates structural and metabolic deterioration. These mechanisms collectively lead to rapid and severe sarcopenia, often developing within days of critical illness. A key clinical concern is the involvement of respiratory muscles, particularly the diaphragm. Diaphragmatic atrophy diminishes ventilatory strength, prolongs mechanical ventilation, and complicates weaning in ARDS patients. Thus, sepsis-induced ARDS and sarcopenia form a self-perpetuating cycle in which respiratory failure accelerates muscle wasting, and muscle loss worsens respiratory insufficiency. This interaction increases ICU stay, disability, and mortality rates. Despite advances in supportive care, effective therapies to prevent or reverse sepsis-associated sarcopenia remain limited. Early mobilization, optimized ventilation, and adequate protein supplementation offer partial benefit but fail to fully counteract underlying catabolic mechanisms. Future translational research should focus on identifying molecular targets to interrupt the cycle of inflammation, mitochondrial injury, and proteolysis driving both ARDS and sarcopenia. A deeper understanding of their shared pathways could lead to novel, mechanism-based interventions that improve survival and long-term functional recovery in critically ill septic patients.
Downloads
Copyright (c) 2025 Georgian Scientists

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.