DIAGNOSTIC DIFFICULTIES AND PECULIARITIES OF TREATMENT FOR ACUTE CARBON MONOXIDE POISONING

Downloads




Carbon monoxide (CO) poisoning frequently presents with nonspecific symptoms resulting in diagnostic delays and misdiagnosis. Severe intoxication can induce stress cardiomyopathy and life-threatening arrhythmias.
Case Presentation: A 35-year-old woman was transferred from a regional hospital with suspected toxic substance exposure. The patient had been found at home in coma; her child was found deceased at the same location. Upon arrival to our facility, the patient developed cardiac arrest with refractory ventricular fibrillation requiring 30 minutes of continuous cardiopulmonary resuscitation and multiple defibrillations. Standard Advanced Cardiac Life Support (ACLS) medications proved ineffective. Administration of magnesium sulfate resulted in successful ventricular fibrillation termination and return of spontaneous circulation.
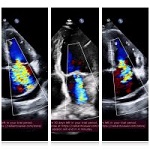
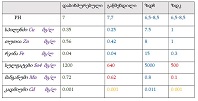
Clinical Findings: Post-resuscitation investigations revealed severe Takotsubo cardiomyopathy with troponin T 4.4 ng/ml (110-fold elevation), creatine kinase >6000 U/L, and critically reduced ejection fraction of 18% with apical akinesia. Hemodynamic instability necessitated maximum vasopressor-inotropic support with norepinephrine, phenylephrine, and dobutamine. The refractory ventricular fibrillation was attributed to critical magnesium deficiency induced by CO toxicity and catecholamine storm.
Management and Outcome: Treatment consisted of high-flow oxygen (FiO₂ 100%), mechanical ventilation, aggressive hemodynamic support, and electrolyte optimization. Complete cardiac recovery occurred within 7 days (ejection fraction 18%→52%). Vasopressors were discontinued on the fifth day, extubation was achieved on the seventh day, with full neurological recovery. The patient was discharged on 16-17th day, with 100% functional recovery and no delayed neuropsychiatric sequelae.
Conclusion: This case emphasizes three critical points: (1) CO poisoning requires high clinical suspicion when multiple household members present with nonspecific neurological symptoms; (2) magnesium sulfate should be considered early in refractory ventricular fibrillation associated with CO poisoning and stress cardiomyopathy; and (3) severe cardiac dysfunction from Takotsubo cardiomyopathy is completely reversible with appropriate intensive support. Magnesium deficiency represents an under-recognized but treatable complication of severe CO intoxication that may prove fatal if unaddressed.
Downloads
Copyright (c) 2025 Georgian Scientists

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.